Hot Flashes


Researchers have identified a group of neurons in the brain’s hypothalamus (brown) responsible for triggering hot flashes, which last between 30 seconds and 5 minutes and strike several times a day. Women are missing work, changing jobs, and turning down opportunities for advancement because of these symptoms, says Stephanie Faubion, director of the Mayo Clinic Center for Women’s Health and medical director of the North American Menopause Society.
Is it possible to cure hot flashes? We may be getting closer.
Nearly all women suffer from hot flashes during menopause. Researchers have finally figured out what triggers them—paving the way for the first new class of treatments since 1941.
:max_bytes(150000):strip_icc()/VWH-ZoeHansen-PostMenopauseHotFlashRiskFactors-Standard-bb923ad5e4d4458a881612330783bbd1.jpg)
Most women experiencing menopause are all too familiar with hot flashes—the sudden onset of fast-rising heat, often accompanied by sweating, heart palpitations, dizziness, fatigue, and/or anxiety—that are much more debilitating than their zippy name suggests.
Up to 80 percent of women report these flashes during menopause, a time when fluctuating and eventually plummeting levels of the hormone estrogen lead to the permanent cessation of menstruation and natural fertility. Hot flashes mimic how an overheating body cools itself, except this is “an inappropriate activation” because body temperature remains in the normal range, says Naomi Rance, a retired neuropathology professor at the University of Arizona College of Medicine and a pioneer in hot flashes research.
Scientists have long been puzzled about this symptom of menopause—also known as hot flushes and vasomotor symptoms—because they didn’t understand exactly what caused a woman to suddenly feel warm. But recently researchers identified a group of neurons in the brain’s hypothalamus responsible for triggering these flashes.
“We always said hot flashes occur because the hypothalamus is malfunctioning, which is true. But we’re now understanding the details about why that is,” says Nanette Santoro, chair of obstetrics and gynecology at the University of Colorado School of Medicine and a longtime menopause researcher.
A drug that blocks the effects of these neurons is currently being reviewed by the U.S. Food and Drug Administration and, if approved, could offer a non-hormonal treatment option as early as 2023. Currently, the primary treatment is menopausal hormone therapy to restore some of the estrogen, but not every woman can safely take these drugs.
The new medicine “would be the first new class of drugs specific to hot flashes” since the estrogen-based treatment Premarin came out in 1941, says Stephanie Faubion, director of the Mayo Clinic Center for Women’s Health and medical director of the North American Menopause Society (NAMS).
More than an annoyance
Women with moderate to severe hot flashes experience them an average of four years, with a third suffering for a decade. These numbers are especially pronounced for Black people and Native Americans. “Women of color tend to have an earlier onset, a longer duration, and the most frequent hot flashes, so the burden is much greater,” says Genevieve Neal-Perry, chair of obstetrics and gynecology at the University of North Carolina School of Medicine who is researching the new medication. Obese women of any ethnicity are also more prone.
After a flash passes—most last between 30 seconds and 5 minutes and strike several times a day—difficulties remain. “There can be a limp dishrag feeling, where people feel a little depleted,” Santoro says. Hot flashes occurring at night are especially problematic because they disrupt sleep.
Women generally enter menopause in the prime years of their careers, making the symptom a professional liability, Faubion says. In one British survey, nearly two-thirds of working women ages 45 to 55 said menopause symptoms rendered them less able to concentrate, and more than half reported losing patience with colleagues and clients. “Women are missing work, women are changing jobs, and women are turning down opportunities for advancement because of these symptoms,” Faubion says.
Everything You Need to Know About Menopausal Hot Flashes
Persistent and frequent hot flashes may also be a harbinger of ill health as some research suggests these symptoms are linked to an increased risk of developing cardiovascular disease, including heart attack, stroke, or heart failure.
Abnormal neurons
Rance’s quest to understand hot flashes began three decades ago, when she was examining microsections of pre- and postmenopausal women’s brains for changes in the hypothalamus—which, together with the pituitary gland promote ovulation and release of sex hormones that control reproduction. She noticed a group of neurons that were swollen in the post-menopausal women. “I had no idea what they were or why they were getting bigger,” she recalls.
She soon located estrogen receptors on the neurons, leading her to hypothesize that the hormone’s absence may have played a role in expanding their size and changing their activity level after menopause. Eventually, her laboratory identified three signaling proteins produced by these neurons: Two, kisspeptin and neurokinin B, were found to have important roles in fertility; the third is dynorphin. The trio were nicknamed KNDy neurons—pronounced “candy”—a play on their initial letters and a nod to the Penn State experts in Hershey, Pennsylvania, who first identified kisspeptin.
Gene discovery indicates motor neurone diseases caused by abnormal lipid processing in cells
Rance’s animal research subsequently revealed how these KNDy neurons regulate temperature. “The neurons send axons to the areas that control body temperature in the hypothalamus,” she says. Since they’re “very, very sensitive to estrogen levels,” when the hormone decreases, KNDy neuron activity increases.
Other researchers working with rodents also connected the neurons to bothersome flashes. Their first challenge: understanding when a mouse is having a hot flash, since you can’t exactly ask, Neal-Perry says.
To address this problem, Neal-Perry’s lab developed a special surface called a thermocline that is cool on one end and warm on the other. Mice placed on the cozy side that were injected with placebo saline remained there. But others receiving capsaicin—a compound in chilis known to trigger hot flashes in humans and animals—scurried to the cool section seeking relief. Finally, a third group of mice were given a drug that activates neurokinin receptors on the KNDy neurons. Like the capsaicin, the drug sent the mice rushing to the cooler side, suggesting it had triggered a hot flash.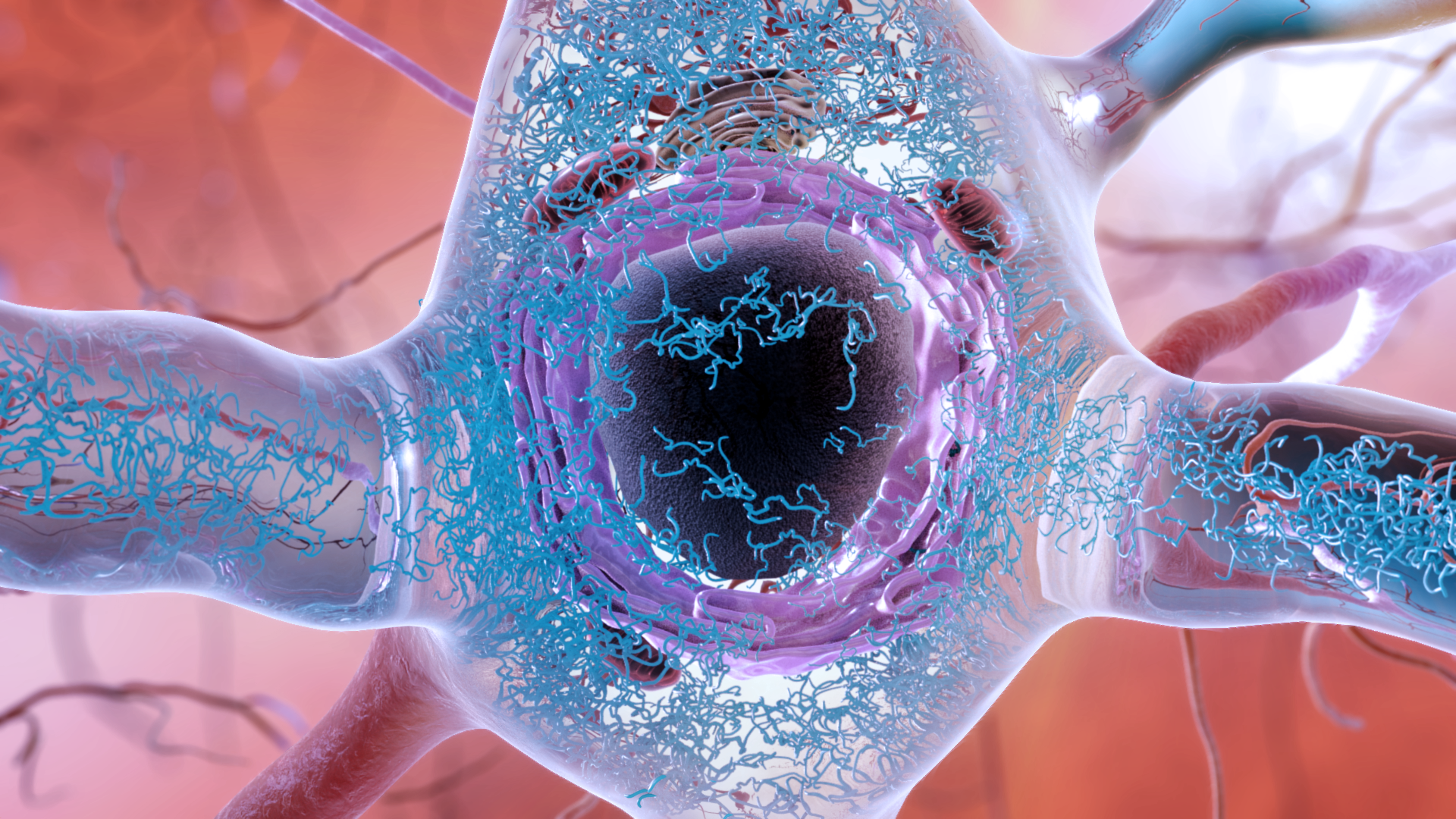
Subsequent studies confirmed neurokinin’s importance in generating hot flashes in women. “In the past decade, we were finally able to put the puzzle pieces together,” Neal-Perry says.
“We shouldn’t be thinking about flushes as an enigma,” as had long been done, Rance says. “We should be thinking about how estrogen affects brain circuits that then influence thermoregulatory pathways.”
Block the peptide, block the flash
In the past few years, companies have begun testing medications that block the receptors on KNDy neurons to reduce hot flashes. Unlike menopausal hormone therapy involving estrogen, the current standard, “this is a well-targeted bullet at the place that’s the problem,” says Santoro, who conducted some of the research.
A small phase 2 clinical trial showed that for women experiencing seven or more hot flashes a day, taking a daily oral drug—fezolinetant, which blocked the neurokinin-receptor—reduced weekly flashes by 45 percent.
At the North American Menopause Society in October, Neal-Perry presented preliminary findings from the phase 3 trial—not yet published in a medical journal—of her fezolinetant research involving more than a thousand women. She reported that women taking the daily pill experienced two to four fewer flashes each day compared to the placebo. Improvements began immediately and continued through the year they were studied, Neal-Perry says. The drug proved equally effective in women of color, whose heavier hot flash burden often makes them harder to treat, she notes.
Another drug that blocks KNDy activity, elinzanetant, is also currently under investigation, with phase 3 trials in progress.
North American Menopause Society
A clinical trial for a third candidate drug, pavinetant, was halted after it caused liver problems. Neither of the other medications triggered similar concerns, Neal-Perry says. In the fezolinetant research, the most common complaint was transient headaches, according to the results presented at NAMS.
FDA approval of a KNDy antagonist would be of particular benefit for menopausal women who cannot safely take hormone therapy or are uncomfortable doing so. While NAMS guidance emphasizes that oral or transdermal estrogen-based treatments are safe for most women under 60 who had their final period within the past decade, that isn’t the case for older women or those who’ve had breast cancer, heart disease, stroke, or a personal or family risk of blood-clotting disorder.
Other future beneficiaries could include men who take drugs for prostate cancer and women on the cancer remission drug tamoxifen, for whom hot flashes are a common side effect, Neal-Perry says. And because KNDy neurons are involved in regulating ovulation, they may ultimately provide a new pathway for infertility treatments, Rance says. Early animal research reveals the neurons’ role in the hormone-based medical condition polycystic ovary syndrome, which can lead to infertility.:max_bytes(150000):strip_icc()/2322667-article-early-signs-of-menopause-5a4cfd9af1300a00373f55f9.png)
Those who treat women for hot flashes are excited about the prospect of a potential new medication. “Having more arrows in the quiver is always good,” Santoro says.
Moreover, women’s health experts are thrilled the scientific confusion behind the flash has finally been resolved. Since nearly all women who reach midlife experience them, Neal-Perry says, “the fact that we haven’t understood the biology of hot flashes until the last decade is pretty amazing.”
Source
https://www.nationalgeographic.com/magazine/article/is-it-possible-to-cure-hot-flashes-menopause-drug
https://www.nhs.uk/conditions/menopause/
https://www.cedars-sinai.org/blog/why-hot-flashes-occur-and-how-to-treat-them.html#:~:text=Hot%20flashes%2C%20also%20known%20as,cause%20chills%20and%20rapid%20heartbeat.
https://molecularbrain.biomedcentral.com/articles/10.1186/s13041-015-0164-4
https://www.menopause.org/